DOI: https://doi.org/10.1038/s41467-025-58362-9
Authors: Isaac Shiri, Giovanni Baj, Pooya Mohammadi Kazaj, Matthias R. Bigler, Anselm W. Stark, Waldo Valenzuela, Ryota Kakizaki, Matthias Siepe, Stephan Windecker, Lorenz Räber, Andreas A. Giannopoulos, George C. M. Siontis, Ronny R. Buechel, Christoph Gräni
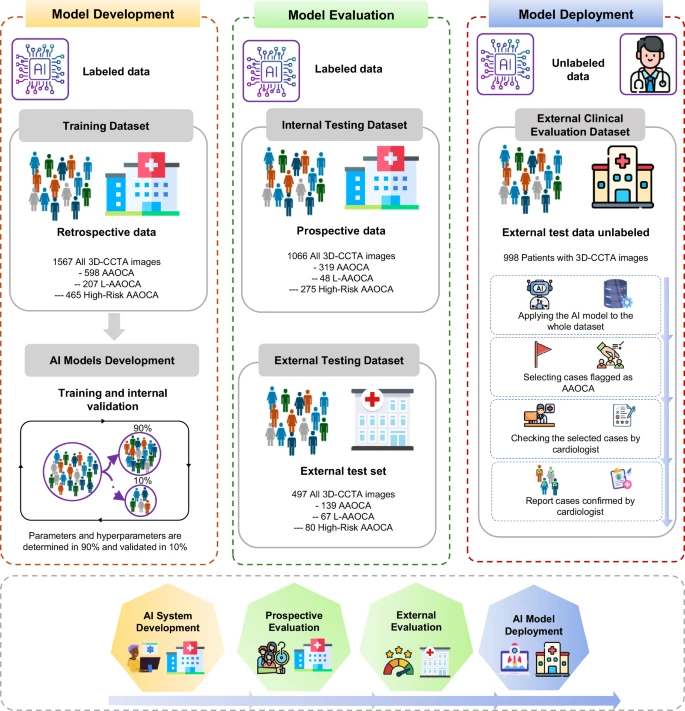
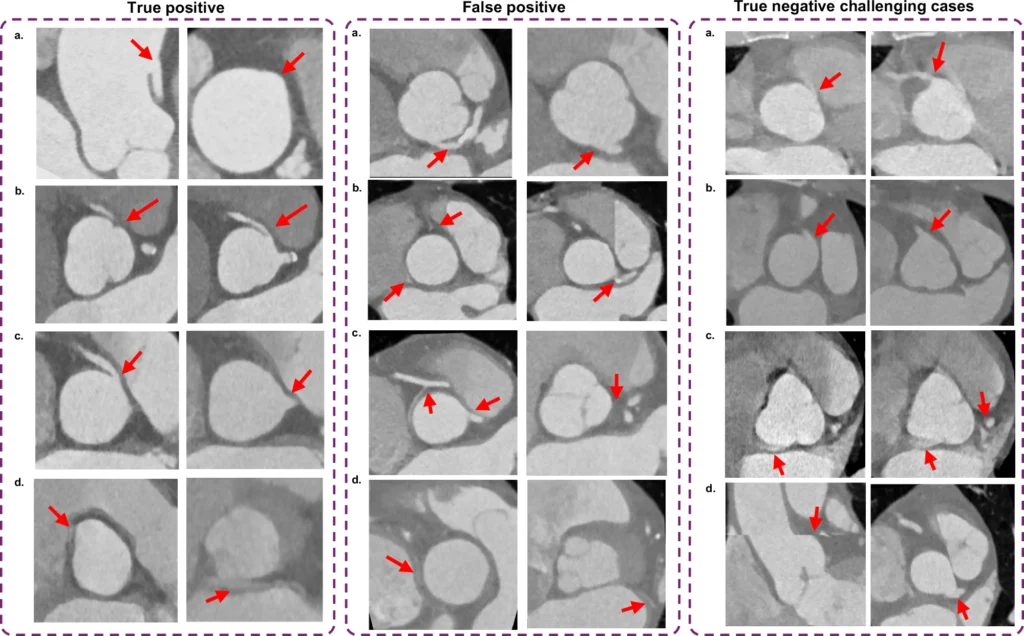
Summary: This study developed a fully automated AI system that detects anomalous coronary artery origins in CT scans with over 99% accuracy, classifies their anatomical risk, and can alert clinicians to potentially life-threatening cases that might otherwise be missed.